 |
|
|
|
| Home > Women Health Concern > Drugs in HRT |
TIBOLONE
-THE NEW SCIENCE OF TISSUE SPECIFICITY Tibolone has often been described as the ideal Hormone Replacement Therapy. This is not true, since there is no "ideal" HRT suitable for all patients. In fact, for peri-menopausal patients and for short term HRT, conventional estrogen is probably better. However for prophylactic long term HRT. Tibolone has advantages that can be best characterized by the term Tissue Specificity"- a new concept in the field of HRT science. It has different pharmacological effects at different target tissues for the overall benefit of the patient. THE NEED FOR TISSUE SPECIFICITY Hormone replacement with estrogen has many beneficial effects in the body, but has some disadvantages, since it affects all estrogen sensitive tissues. The greatest concern is the fact that estrogens stimulate the endometrium. This means that estrogen could increase the risk of endometrial cancer, unless they are taken in combination with a progestogen, needed to protect the endometrium by including a regular shedding of the endometrium, and resulting in a withdrawal bleed. In addition, estrogens stimulates receptors in breast tissue which can induce breast tenderness. Moreover, long-term, use is potentially associated with a slight, albeit small, increased risk of breast cancer. Both these problems have proven to be major obstacles to the long-term use of conventional HRT. So postmenopausal women, are not able to take advantage of estrogen's proven benefits against osteoporosis, heart disease, and possibly Alzheimer's disease. MECHANISMS OF BIOCHEMICAL TISSUE SPECIFICITY Tibolone is a synthetic steroid which is metabolized in the body into three active metabolites. These molecules differ in their ability to bind to estrogen, progestogen and androgen receptors. Tibolone can be broken down into its metabolites at the level of individual tissues, which means the action of Tibolone at an organ system depends on the metabolic conversion in that specific tissue. (See Table 2). CLINICAL ACTION OF TIBOLONE ON VARIOUS TISSUES
TIBOLONE AND BONE
TIBOLONE AND ENDOMETRIUM
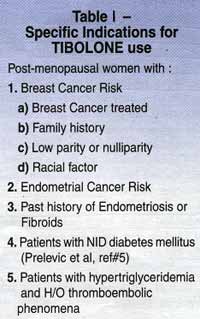
TIBOLONE AND BREAST TISSUE Unlike conventional HRT, women using Tibolone rarely complain of breast tenderness. No evidence of carcinogenecitiy for preclinical studies of Tibolone. In cell cultures, Tibolone and its metabolites are very potent inhibitors of the stimulation of breast tumours. SUMMARY Among the products available in India at present, Tibolone comes close to being the ideal product, for long term HRT. The fact that it induces amenorrhoea in most cases, providing menstruation free HRT, is most welcome to Indian women. Side effects do occur in a minority of women increased body weight, dizziness, headache, hirsutism, oedema and rashes have been reported. The major deterrent factor for Tibolone use in India is probably the cost due to which it may have to be used in selected patients. Table 1 is an attempt to list those conditions where Tibolone could be used for special indications.
SELECTIVE ESTROGEN RECEPTOR MODULATORS (SERMS) The current concept of ER action includes a rheostat like action of the receptor due to conformational changes in the ligand receptor complex that depend on the nature of the bound ligand. This conformational change also determines subsequent adaptor protein interactions. Recognition of the tissue-specific activities of tamoxifen the first selective ER modulator (SERM) led to the development of new SERMS (Taloxifene and toremiphene). SERMS bind to estrogen receptors and act like estrogen in some tissues (agonist effect). In other tissues, they block the effects of estrogen (antagonist effect). 1.) Tamoxifen reduced the risk for invasive breast cancer by 49% among women of all ages (P .002) and the risk for estorgen receptor positive tumors by 69% while ER negative tumors were not affected. EFFECTS OF TAMOXIFEN ON BONE MINERAL DENSITY (BMD) That spinal BMD in tamoxifen treated women increased by 0.61% per year (P=0.04) THE EFFECT OF TAMOXIFEN ON LIPID PROFILE AS WELL AS ON THE CARDIOVASCULAR SYSTEM ? Cardioprotective it has a favorable impact on lipid profile among post menopausal women-there was a decrease in total cholesterol by 7-17%, and a decrease in LDL cholesterol by 6-29%. Few studies have shown an increase in HDL. Lower rates of myocardial infarction higher rate of thromboembolism. TAMOXIFEN & ADVERSE EVENTS Upto 25% of patients On Tamoxifen have hot flashes and nausea and vomiting. Vaginal bleeding or discharge as well as menstrual irregularity is seen. In the Breast Cancer Prevention Trial (BCPT), Tamoxifen increased the risk of pulmonary embolism by 3.01% CI, 1.15-9.27) and risk of deep vein thrombosis by 1.60-3.0(95% CI 0.91-2.86) as compared toplacebo. In the BCPT STUDY, tamoxifen treated women were 2.53 times more likely than those in placebo group to develop endometrial cancer(95% Cl 1.35-4.97%) The risk was much greater among women 50 years and older. Visual disturbances including cataracts, retinoparthy, corneal changes and hypercalcemia have been associated with tamoxifen. 2.) Raloxifene is a benzothiophene derivitive. It is used for treatment and prevention of osteoporosis in postmenopausal women. The dosage is 60 mg tablet once daily and may be taken anytime of the day without regard to meals. The effects of raloxifene on total hip and total body BMD. weresimilar to the effects of HRT and alendronate sodium (5mg) Raloxifene reduces vertebral fracture risk by 30 %among women with preexisting fractures and by 50% among women without preexisting fractures. RALOXIFENE AND CARDIOVASCULAR RISK Raloxifene improved several markers of cardiovascular risk including total and low density lipoprotein cholesterol, fibrinogen, lipoprotein (a) and hemocysteine levels without increasing triglycerides or c-reactive protein levels in healthy postmenopausal women with osteoporosis. RALOXIFENE-EFFECTS ON THE BREAST In clinical trials comparing raloxifene (60mg daily) to continuous or cyclic HRT, raloxifene was associated with significantly less breast pain. RALOXIFENE & ENDOMETRIUM Raloxifene was not associated with vaginal bleeding, endometrial proliferation or an increased risk for endometrial cancer. OTHER ADVERSE EFFECTS Hot flashes were reported in the first 6 months of treatment with raloxifene but discontinuation rates did not differ between raloxifene and placebo. Leg cramps and influenza-like symptoms are also reported. In the MORE trial raloxifene increased the risk for venous thromboembolic events including deep vein thrombosis and pulmonary embolism (R.R. 3.1, 95% CI 1.5-6.2). This risk is similar in magnitude to that found with HRT use. Toremifene is used for its effects on breast tissue and has a stimulatory effect on the uterus and endometrium. There seems to be and increased risk of thromboembolic events with continuous use of this SERM. CONCLUSION Tamoxifen is indicated for breast cancer treatment and is not recommended for longer than 5 years as adjuvant therapy. It is recommended for reduction of breast cancer among healthy women at risk for this condition. Candidates for tamoxifen chemoprophylaxis include women who:
Phytestrogens are naturally occurring plant sterols which have an action similar to estrogen. Phytestrogens can be classified into 3 groups. 1. Isoflavones : e.g. genistein and diadzin Sources: soy, garbanzo beans and other legumes. 2. Lignans : are components of plant cell wall and become activated after action of intestinal bacteria on grains, Seed oils, particularly flaxseed are rish sources of lignans. 3. Coumestans: red clover, sunflower seeds and bean sprouts. POPULATION BASED STUDIES Phytestrogens may potentially confer health benefits related to cardiovascular diseases, cancer, osteoporosis and menopausal symptoms. These potential health benefits are consistent with epidemiological evidence that in countries such as China and Japan where the local diet is rich in soy foods and the intake of legumes 50-90 gms/person/day, the incidence of various cancers, heart disease and osteoporotic fractures is less. MECHANISM OF ACTION American and European diets tend to increase plasma level of sex hormones and decrease SHBG. Thus the level of sex hormones to which tissues are exposed is very high predisposing the women to malignancies. Diet rich in soy foods (Phytestrogens) decreaset he LH levels and also reduces estrogen levels through various mechanisms. They modify the hormone production and hormone metabolism thus limiting the cancer growth. The mechanism by which phytestrogens produce biological and clinical effects is most likely related to an ability to bind to the estrogen receptor due to structural similarity to estrogen.Phytestrogens also have a lipid lowering effect but the exact mechanism of action is not known. Probably there is an increase in bile acid excretion and also LDL receptors thus leading to increased removal of cholesterol. They also alter secretion of thyroxine, insulin and glucagon. Phytestrogens decrease hot flushes and improve vaginal cytology in postmenopausal women. Like isoflavanes and lignans, phytestrogens have antioxidant activity.
EPIDEMIOLOGICAL ASPECTS : Reproduction - Phytestrogens may cause anovulation and increase menstrual cycle length. A few animal studies have been done but there are no human studies as yet. Breast Cancer
- Estrogen is known to promote breast cancer. Phytestrogens
relieves postmenopausal symptoms without stimulating breast
tissue. In fact phytestrogens are known to inhibit the growth of
several cancer cell lines including breast cancer cell lines. Osteoporosis - Phytestrogens (Ipriflavone) cause decreased bone resorption and enhances osteoblast function. The mechanism of action is unclear. Cardiovascular disease - Several lines of evidence including epidemological, clinical trial data and basic science suggest a well established role of phytestrogens in decreasing the risk of cardiovascular diseases. This is because of the cholesterol lowering effect .
VARIOUS TRIALS CONDUCTED WITH MEDICINAL BOTANICALS 1. Black Cohosh (cimicifuga racemosa) This contains an active compound which does not have ability to bind to ER but decreases LH levels after chronic treatment. 2. Dong quai (angelica polymorpha maxim) This is the most commonly prescribed Chinese herbal medicine. This is used to regularize menstrual cycles. But studies have not shown any estrogen like effect. 3. Evening
primrose : 4. St. Johns' wort (hupericum perforatum) This has been used for centuries to treat mild to moderate depression. 5. Valerian root (VBaleriana officianlis) This has been used
for ages as a tranquillizer. There are many more herbs
which help to relieve post menopausal symptoms.e.g. Nettle (utrica
diocia) used in postmenopausal bleeding due to senile vaginits.
CONCLUSION Increasing consumption of soy, soy products and plant based foods, in general is consistent with current recommendations to increase fibre and antioxidant intakes and replacing sources of saturated fat and cholesterol in diet. Previous << HORMONE REPLACEMENT THERAPY (HRT)
|